Cannabis and Anxiety: What the Research Actually Shows About Mechanism, Dose, and Variability
Anxiety is the single most common mental health reason consumers turn to cannabis. It is also where most consumers get burned. Here is what the past three years of research actually shows about mechanism, dose, terpenes, and individual variability.
Anxiety is the single most common mental health reason consumers turn to cannabis. It is also the place where most consumers get burned. The same product that calms one person makes another spiral. The same person who finds calm at 5 mg of THC finds dread at 12.5 mg. The label says "indica" or "calming hybrid" and tells you almost nothing about what it will actually do.
This is not a problem you fix with a better strain name. It is a problem you fix with a better question.
Here is what the past three years of research has actually figured out about cannabis and anxiety, and how to apply it to your own use.
The mechanism is real, and it is not just THC
Cannabidiol, the non-intoxicating cannabinoid, was puzzling for a long time. It does not get you high. It does not produce the classic cannabinoid receptor activation pattern. So how does it actually do anything?
A 2025 review in Biochemical Pharmacology gave the cleanest answer to date. CBD is a modest-affinity agonist at the 5-HT1A serotonin receptor. The 5-HT1A receptor is the same target hit by SSRIs and buspirone, two of the most prescribed anxiolytics. CBD's anxiety-reducing effects in animal models can be reliably blocked by 5-HT1A antagonists. That is the kind of evidence that turns a hypothesis into an actual mechanism.
CBD also inhibits FAAH, the enzyme that breaks down anandamide, your body's natural endocannabinoid. Inhibit FAAH and anandamide tone stays elevated longer, which is associated with calmer baseline state. Two pathways, neither requiring euphoria.
What does this mean in practice? It means CBD's mechanism is no longer hand-waving. It is a real serotonergic and endocannabinoid effect, with all the dose-dependence and individual variation those pathways imply.
Important: this does not mean CBD replaces an SSRI. It means we finally know what CBD is actually doing.
(Source: Biochemical Pharmacology, 2025.)
The dose curve is biphasic. Low calms. High agitates.
This is the single most actionable finding in cannabis-anxiety research, and it is consistent across animal and human work.
A controlled human study of 42 participants compared 7.5 mg vs 12.5 mg oral THC. Same compound. Same product. Different dose. The 7.5 mg group reported significantly lower anxiety than placebo. The 12.5 mg group reported significantly higher anxiety than placebo. Same direction of effect, opposite outcome, just by changing the dose.
A separate 2022 review in Cannabis and Cannabinoid Research compared THC-dominant cannabis to a 1:1 THC to CBD ratio chemovar in healthy adults. The 1:1 ratio induced significantly less state anxiety than THC alone, even though both contained the same THC dose.
The lesson is not "take exactly 7.5 mg." The lesson is the principle:
- More THC is not better.
- CBD alongside THC blunts the anxiety risk.
- Your personal threshold sits somewhere on this curve and you do not know where without testing.
The advice "start low and go slow" used to be folklore. Now it has clean human RCT support.
(Source: Cannabis and Cannabinoid Research, 2022 to 2023.)
Terpenes do something. Limonene specifically softens THC anxiety.
Terpenes are the aromatic molecules that give cannabis its scent. For years, the industry treated them as marketing copy. Recent work has started treating them as pharmacology.
A 2024 double-blind crossover trial out of Johns Hopkins and CU Boulder isolated d-limonene and tested it head-to-head with THC alone in healthy adult volunteers. Participants vaped vaporized THC plus d-limonene on one day and THC alone on another. Self-reported anxiety dropped by approximately 45 percent when limonene was in the mix. Subjective intoxication did not drop. The pleasant effects of THC were preserved. The anxiety was not.
That is rare evidence in this field. A specific terpene, isolated, tested in humans, with a clear effect on a specific symptom dimension.
What this means: the terpene profile of a product is not decoration. It can shift the anxiety risk of the same THC dose. Future product selection that ignores this is leaving usable signal on the table.
Caveat: this was a healthy-adult study, not a clinical anxiety population. We do not yet know if limonene helps an anxiety disorder. We know it shifts the THC anxiety side effect. That alone is meaningful.
(Source: Drug and Alcohol Dependence, 2024.)
The same product can feel different on different days. That is not random.
If you have ever wondered why a product that worked beautifully one week made you wired the next, the explanation is probably not your imagination.
Research suggests estrogen, the dominant female sex hormone, inhibits FAAH, the enzyme that breaks down anandamide. When estrogen is high, anandamide stays elevated longer, and your endocannabinoid tone shifts toward calmer baseline. When estrogen drops, FAAH is uninhibited, anandamide drops faster, and baseline tone shifts the other way. The effect is a body-clock pharmacology that operates on top of whatever you consumed.
The same logic applies in different forms across other hormonal contexts: stress, sleep deprivation, alcohol, even hydration. Your endocannabinoid system has set points. They move.
This is the kind of pattern that no population study can detect, because every other person in the study has a different set point and a different schedule. Only your own log, with the dates included, can tell you when your own anxiety response shifted, and what you consumed at the time.
(Source: Addictive Behaviors, 2025.)
The bridge between any of this and your own outcome is your data
Smart Cannabis, a 2025 prescription digital therapeutic framework published in ScienceDirect, modeled a closed loop: scanned chemistry in, symptom logs in, machine-learning recommendations out. The Releaf App Florida study, published in 2024, gave that loop a real-world test. Several hundred Floridians logged their anxiety and depression symptoms before and after cannabis use. The app's data showed that within roughly two weeks of consistent logging, individual signal emerges. Anxiety and depression users reported greater symptom relief than pain users.
Two weeks is the operative number. Not six months. Not three sessions.
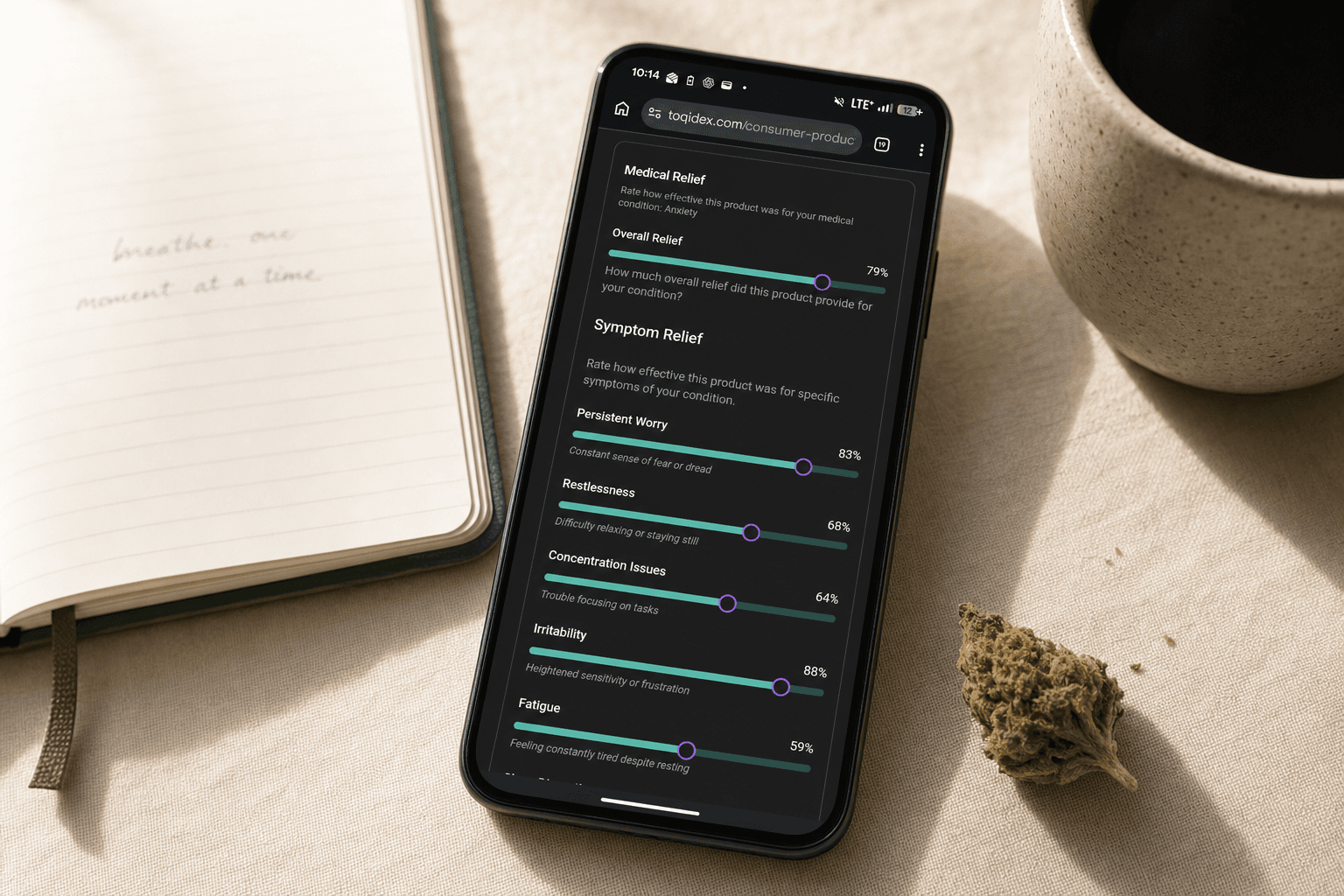
This is exactly the loop TOQidex was built for. Scan a product, the system extracts the chemistry. Set anxiety as your tracked medical condition and you unlock the dedicated symptom-relief panel: an Overall Relief score, plus ten specific symptoms (Persistent Worry, Irritability, Restlessness, Fatigue, Concentration Issues, Sleep Disruption, Muscle Tension, Increased Heart Rate, Appetite Changes, Social Withdrawal). Score each after a session, alongside the standard recreational coefficients for session-feel context.
Two things to know about how the model works. The 8 recreational coefficients (Anxious vs Calm, Sleepy vs Energetic, and the rest) come with founder-trained predictions from day one, so you get useful signal even before you have a personal model. The medical-condition models do not. Anxiety symptom predictions train only on your own logged data, and they unlock after ten unique products. Until then, you are building the dataset. After, you are getting predictions about you, not the average user. The system can correlate which cannabinoids and terpenes track to which of your specific symptoms. Not a single anxiolytic verdict, but eleven resolved signals the strain name was never going to give you.
The cannabis industry spent the last decade arguing about whether sativa or indica was more "anxiolytic." It was the wrong question. The right question is: which cannabinoids and terpenes correlate with your best outcomes? Your log is the only place that question gets answered.
(Source: Cannabis (UCF), 2024; Smart Cannabis, ScienceDirect, 2025.)
How to apply all of this
The science gives you principles. Your log gives you specifics. The intersection is where intentional cannabis use lives.
The principles are simple. More THC is not better, and the 7.5 versus 12.5 mg study should sit in the back of your head every time you think about dose. A ratio closer to 1:1 THC to CBD blunts the anxiety risk that THC alone carries. Limonene in the terpene profile is signal worth noting, not marketing copy. And the same product can feel different on different days, because your endocannabinoid set points move with hormones, sleep, and stress, so the dates in your log matter as much as the products.
The specifics only show up when you write them down. Population studies cannot tell you what your own response curve looks like, because every other person in the study is on a different curve. The Florida Releaf data and the Smart Cannabis modeling both pointed to roughly two weeks of consistent logging as the point where individual signal starts to emerge. Two weeks. Not six months.
That is the loop TOQidex was built around. Scan the product, the system extracts the chemistry. Log what happened. Over enough sessions, the cannabinoid and terpene patterns that track to your best outcomes become legible, instead of hiding behind the strain name.
Cannabis does not treat anxiety. It interacts with anxiety pathways in measurable ways, and those interactions vary by person, dose, ratio, terpene profile, and the day of the cycle you happen to be on. The difference between a marketing claim and a useful tool is whether you have the data to tell them apart.
Your log is the tool.
For more on the framework behind the recreational coefficients, see toqidex.com/blog/8-coefficients-of-cannabis.
Track Your Own Experience
TOQidex helps you build a personal evidence base by tracking your cannabis experience against real product chemistry.
Start Tracking FreeTOQidex tracks user-reported symptom response. It does not diagnose, treat, cure, or prevent any condition. All outputs reflect probability based on your personal logged data. This article is for informational purposes only and does not constitute medical advice.